Table of Contents >> Show >> Hide
- Why aging eyes lose “HD” vision
- Geographic atrophy: what “irreversible” really means
- The breakthrough: a tiny retinal implant + smart glasses
- What the clinical results showed (and what they didn’t)
- How this fits with today’s GA treatments
- Who might be a candidate for a retinal implant system?
- Practical examples of what “restored” can look like
- Frequently asked questions
- Experiences: what it’s like living with GAand adapting to an implant (about )
- Takeaway
Aging does a lot of rude things. It steals your knees, your ability to eat pizza at midnight without consequences, andif you’re one of millions of peopleyour sharp, straight-ahead vision. For many older adults, the culprit is age-related macular degeneration (AMD), and one advanced form called geographic atrophy (GA) has long carried a particularly grim label: irreversible.
But “irreversible” doesn’t always mean “nothing can be done.” It can also mean “the original tissue won’t grow back”… while technology quietly slips in through the side door with a workaround. In late 2025, researchers reported that a tiny wireless retinal implant paired with special glasses helped many people with GA regain useful central visionenough to identify letters and read again. That’s not a full rewind to 20/20, but for someone who’s been living with a blank spot in the center of everything, it can feel like getting the middle of life back.
Why aging eyes lose “HD” vision
Your retina is like a living camera sensor lining the back of the eye. And your macula is the tiny, high-performance center of that sensor responsible for sharp detail: reading, recognizing faces, threading a needle, and spotting the difference between “salt” and “sugar” before your coffee becomes a science experiment.
AMD happens when aging-related changes damage the macula over time. Early AMD may cause few symptoms, but as it progresses, central vision gets blurry or distorted. Straight lines can look wavy. Letters can fade or break apart. Eventually, a dark or blurry spot can take up residence in the center of what you seelike a thumbprint on the world.
Dry vs. wet AMD (and why GA is the “dry” nightmare level)
AMD comes in two major types:
- Dry AMD: More common. Progresses gradually. In late stages, it can lead to geographic atrophy, where patches of retinal cells die.
- Wet AMD: Less common but often more sudden and severe. Caused by abnormal blood vessels and typically treated with anti-VEGF injections.
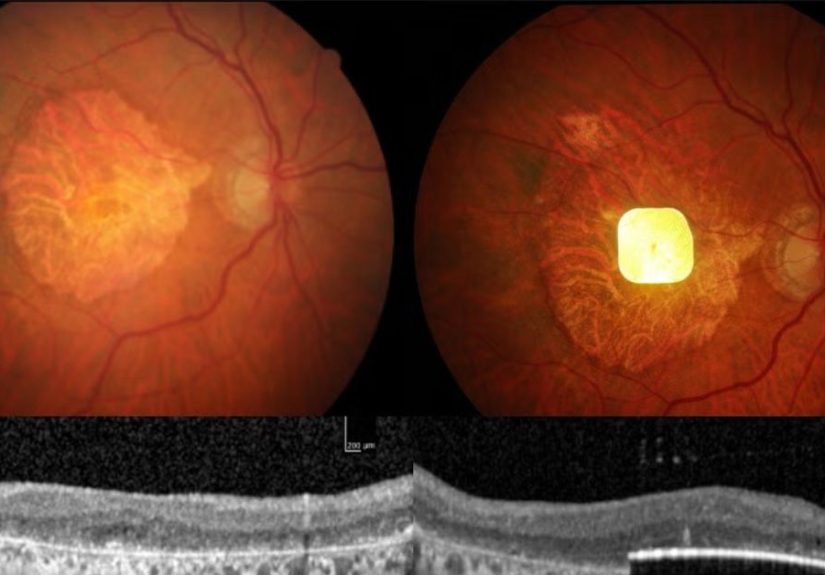
GA is part of advanced dry AMD. It’s called “geographic” because the areas of atrophy can look like irregular map shapes on retinal imaging. As these patches enlarge and creep toward the fovea (the macula’s bullseye), the brain loses access to crisp central information.
Geographic atrophy: what “irreversible” really means
In GA, the damage isn’t just inflammation or swelling that might calm down later. Cells in the outer retina and supporting layers are lost. When those cells are gone, the body doesn’t simply replace them the way it heals a cut on your skin. That’s why GA has historically been framed as permanent central vision loss.
Important nuance: permanent doesn’t always mean total darkness. Many people keep peripheral vision for a long time. The painful part is that central vision is the vision we use for most daily “precision tasks”: reading medication labels, recognizing faces, driving (often no longer safely), and navigating unfamiliar spaces without feeling like you’re playing life on “hard mode.”
How common is it?
AMD is common in the U.S., and GA affects roughly around a million Americans. Risk rises sharply with age, especially after 60. So yes, this is a “big deal” condition, not a rare medical trivia answer.
The breakthrough: a tiny retinal implant + smart glasses
The exciting news isn’t that GA suddenly became reversible. The exciting news is that researchers built a system that can bypass the missing photoreceptors and deliver a new kind of central vision signal through remaining retinal circuitry.
One of the most discussed systems is the PRIMA photovoltaic retinal implant. It’s a microarray chip placed under the retina in the region where GA destroyed natural light-sensing cells. A pair of specialized glasses captures the scene in front of you and projects it onto the implant using near-infrared light. The implant converts that light into tiny electrical stimulation patterns, activating remaining inner retinal neurons, which then send signals through the optic nerve to the brain.
“Wireless” doesn’t mean Bluetooth eyeballs
When people hear “wireless eye implant,” they imagine a tiny Wi-Fi router behind the eyeball, streaming Netflix straight into the visual cortex. Reality is less sci-fi, but still impressive.
The system is considered wireless because there’s no cable running out of the eye and no implanted battery pack that needs charging like a phone. Instead, the glasses deliver energy and information through light (near-infrared) to power the implant’s stimulation. In other words: the glasses do the heavy lifting, and the implant does the precise, microscopic “tap-tap-tap” signaling.
What kind of vision does it restore?
Think “functional central vision,” not “perfect vision.” People often describe prosthetic vision as:
- Lower resolution than natural sight (more like pixels than photographs)
- High contrast (letters and shapes can become identifiable)
- Different processing (the brain needs training time to interpret the new signal)
That training part matters. This isn’t like flipping on a light switch. It’s closer to learning a new accentyour brain can understand it, but it takes practice.
What the clinical results showed (and what they didn’t)
In a multicenter clinical study of people with GA due to AMD, participants received the implant and were tested at 6 and 12 months with and without the PRIMA glasses. The key question: did vision improve in a meaningful way when the system was used?
The headline result
Among participants who completed 12 months of follow-up, a large majority achieved a clinically meaningful improvement in visual acuity when using the PRIMA system. That’s the phrase researchers use when improvement isn’t just “technically measurable,” but likely to matter in real life.
Safety and side effects
Any implant surgery inside the eye is serious business. Reported serious adverse events occurred, and many happened in the early post-surgery period. The reassuring signal in the data was that most resolved, and average peripheral (natural) vision remained about the same as baseline. Still, “resolved” doesn’t mean “fun,” and anyone considering this kind of technology should expect close monitoring, follow-up visits, and a real recovery period.
What this study does NOT prove
- It doesn’t cure AMD or GA. The underlying disease process still exists.
- It doesn’t restore normal eyesight. It provides a new form of central vision signal.
- It doesn’t guarantee driving vision. Regulations and safety depend on many factors, including contrast sensitivity and field testing.
- It’s not for everyone. Trial criteria were specific; real-world candidacy will likely be, too.
How this fits with today’s GA treatments
Before we talk “bionic vision,” it helps to zoom out: what can people do right now if they have GA? In 2023, the U.S. finally got FDA-approved medications for GA that can slow the growth of atrophy lesions. That’s progressbut slowing damage is different from restoring function.
Complement inhibitor injections: slowing the map from spreading
Two FDA-approved drugs for GA secondary to AMD are:
- Syfovre (pegcetacoplan)
- Izervay (avacincaptad pegol)
These medications are given by intravitreal injection (an injection into the eye), typically on a regular schedule. Their goal is to slow GA lesion growthnot to bring dead retinal cells back. For some patients, that means buying time: preserving usable vision longer, delaying the day the atrophy reaches the fovea, or slowing how fast the blind spot expands.
The trade-off is that injections require commitment and monitoring, and like all eye injections, they can carry risks such as inflammation, infection (rare but serious), and other complications. Your retina specialist is the person who can turn this from “internet info” into “personalized decision.”
Low-vision rehab: the underrated superpower
Whether you use medications, an implant, or neither, low-vision rehabilitation can be life-changing:
- High-contrast reading strategies (lighting, bold fonts, contrast filters)
- Optical aids (magnifiers, telescopic glasses)
- Electronic aids (tablet settings, screen readers, wearable devices)
- Home modifications (labels, organization systems, glare control)
Many people wait too long to ask for this help. Don’t. Low vision specialists exist to help you keep doing the stuff you care aboutsafely and independently.
Implantable miniature telescope: an older “implant” option
Not all vision implants are electronic. The implantable miniature telescope (IMT) is an FDA-approved device (placed inside the eye) designed for certain people with end-stage AMD. It works like built-in magnification, enlarging the central image so it lands on healthier retinal areas around the damaged macula.
The IMT can improve function for select patients, but it also comes with trade-offs (including reduced field of view in the implanted eye) and requires rehabilitation training. It’s not the same thing as a retinal microchip system, but it’s part of the bigger story: ophthalmology has been trying to give central vision back for a long timeand now the toolbox is expanding.
Who might be a candidate for a retinal implant system?
Final candidacy rules will evolve as trials expand and regulators weigh benefits vs. risks. But based on how these studies are designed, likely requirements include:
- Advanced GA from AMD with severe central vision loss
- Enough remaining inner retinal function to carry the signal onward
- Stable eye health without conditions that would make surgery or outcomes riskier
- Willingness to train (this is a “rehab required” technology)
A key mindset shift: this isn’t just “get implant, go home, read War and Peace.” It’s more like “get implant, do structured practice, retrain the brain, then gradually reclaim tasks.”
Practical examples of what “restored” can look like
“Restored vision” can sound like a miracle headline, so let’s ground it in everyday wins. For someone with GA, examples of meaningful improvements might include:
- Reading large-print text without guessing every third letter
- Seeing the high-contrast numbers on a microwave or phone keypad
- Recognizing a spouse’s face at conversational distance (especially with good lighting)
- Finding the center of a plate and eating without the “fork-to-nowhere” problem
- Doing puzzles againcrosswords, Sudoku, word searchesbecause the symbols stop disappearing into the blind spot
These aren’t trivial. They’re the difference between “I need help” and “I’ve got this.”
Frequently asked questions
Is this a cure for geographic atrophy?
No. GA still involves permanent loss of certain retinal cells. The implant is best described as a prosthetic approacha way to deliver visual information through remaining retinal pathways.
Will it bring back color vision?
Prosthetic vision systems typically focus on contrast and shape. Color may not be restored in a natural way, depending on the technology. Think “useful detail,” not “perfect color photography.”
Do you still need glasses?
Yes. In the PRIMA-style approach, the glasses are a core part of the system: they capture and project the image that the implant translates into stimulation. Without them, the implant isn’t delivering the same “information stream.”
Is it available everywhere in the U.S.?
Availability depends on regulatory approvals and clinical trial access. Many cutting-edge implants start in specialized centers and expand over time. If you’re interested, a retina specialist can help you check legitimate trial listings and referral pathways.
What should families know?
Expect a learning curve. Support matters: rides to appointments, help with practice routines, and patience while the brain adapts. The right kind of encouragement can speed up progress more than you’d think.
Experiences: what it’s like living with GAand adapting to an implant (about )
If you’ve never had central vision loss, here’s the weird part: you can still “see,” but you can’t see what you’re looking at. You turn your head directly toward a face…and the face drops into the blind spot like it’s dodging you on purpose. People with GA often describe becoming experts at looking slightly away from what they want to see, using healthier retina off to the side. It’s like trying to read a sign by staring at the sidewalk next to it. It works sometimes. It’s exhausting always.
Day-to-day experience tends to come in waves. Good lighting days feel like small victories. Dim restaurants feel like visual escape rooms. Grocery stores become a mix of confidence (“I know this aisle”) and surprise (“Why is every label the same color?”). Many people also report a sneaky emotional layer: grief for independence, frustration with constant asking, and the fear that the blur will keep expanding. Those feelings are normal, and they deserve as much attention as the medical chart.
When someone tries an advanced devicewhether it’s a wearable electronic magnifier, a telescope implant, or an investigational retinal microchipthere’s often a similar pattern: hope, then awkwardness, then practice, then progress. Early on, the brain may interpret the new input as unfamiliar: shapes look “blocky,” letters feel incomplete, and it can be tiring to use the system for more than short sessions. This is where structured training matters. Rehabilitation specialists commonly encourage short daily practice windows, high-contrast materials, and clear goals: “Read three letters,” then “read a word,” then “read a line,” then “read a text message.” Tiny steps are not tiny when you’ve been locked out of the center of the page.
Families often notice changes before the patient does. The first time someone stops reaching past a cup and grabs it cleanly, that’s a moment. The first time they read a grandchild’s birthday card without handing it off, that’s a moment. Even when the vision isn’t “normal,” it can become usefuland usefulness is what restores dignity.
It’s also common for people to blend strategies. Someone might use GA-slowing injections to preserve what’s left, rely on low-vision tools for everyday tasks, and explore an implant option if they’re eligible and motivated for the training. In real life, eye care isn’t one dramatic intervention. It’s usually a smart stack of solutions.
The most consistent experience reported by patients who benefit from these technologies is not “I got my old eyes back.” It’s: “I got pieces of my life back.” And honestly, at a certain age, that’s the kind of upgrade worth talking about.
Takeaway
Geographic atrophy has long been one of the most discouraging age-related eye conditions because it destroys the cells responsible for sharp central vision. Today, that story is changing. FDA-approved drugs can slow progression, and emerging implant technologies suggest something even more ambitious: giving people with GA a new route to central vision through prosthetic signaling.
If you or a loved one is facing GA, the best next step is practical, not viral: schedule a retina specialist visit, ask about current treatment options, and discuss whether clinical trials or advanced low-vision programs make sense for your goals. “Irreversible” may still describe the biologybut it doesn’t have to describe the future.