Table of Contents >> Show >> Hide
- What Exactly Is a Drug-Eluting Stent?
- How Drug-Eluting Stents Work (The “Tiny Pharmacy” Breakdown)
- How a Drug-Eluting Stent Is Placed (Step-by-Step, Human Version)
- Why DES Usually Reduce Repeat Narrowing (And Why That Matters)
- Risks and Tradeoffs: The Two Big WordsClotting and Bleeding
- Who Might Get a Drug-Eluting Stent?
- Recovery and Long-Term Care: What Helps a Stent “Age Gracefully”
- Frequently Asked Questions
- Key Takeaways
- Experiences: What It’s Like in Real Life (Patients, Families, and Clinicians)
Imagine a tiny metal spring that props an artery open and comes with its own slow-release “anti-drama”
medicinelike a bouncer and a peace negotiator rolled into one. That’s the basic vibe of a
drug-eluting stent (DES).
Drug-eluting stents are used most often during percutaneous coronary intervention (PCI)
(also called angioplasty with stenting) to treat narrowed or blocked coronary arteries.
Their claim to fame: they keep blood flowing while releasing medication over time to reduce the chance the
artery narrows again (a problem called restenosis).
What Exactly Is a Drug-Eluting Stent?
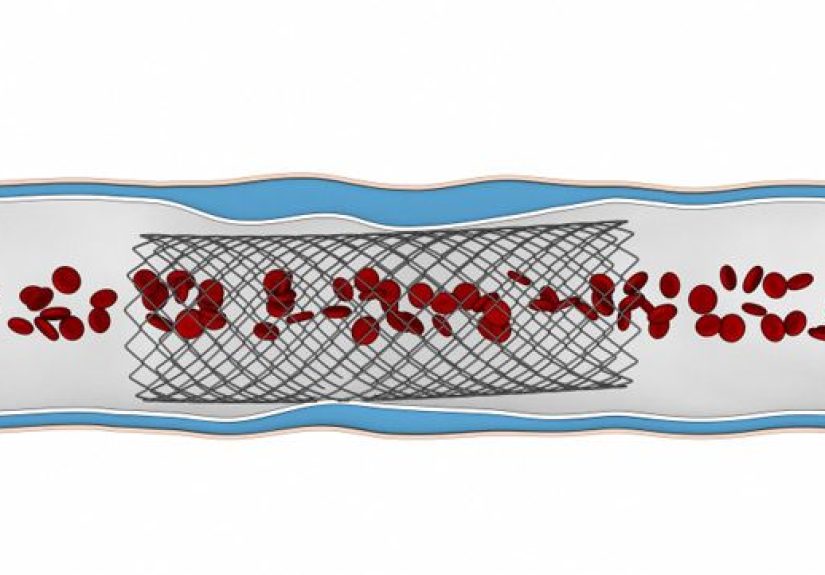
A stent is a small, expandable mesh tube placed inside an artery to help keep it open. A
drug-eluting stent is a stent that has a coating containing medication that is released
gradually into the artery wall after placement. The goal is to reduce excessive tissue growth during healing.
DES vs. Bare-Metal Stents (BMS): What’s the Difference?
Both DES and bare-metal stents act like scaffolding, physically supporting the artery. The main difference is
the coating:
| Feature | Drug-Eluting Stent (DES) | Bare-Metal Stent (BMS) |
|---|---|---|
| Main purpose | Keeps artery open + releases medication to reduce re-narrowing | Keeps artery open (no drug coating) |
| Restenosis risk | Generally lower | Generally higher |
| Medication after stent | Often requires careful antiplatelet therapy planning | Also requires antiplatelet therapy, sometimes with different duration considerations |
| Common today? | Very common | Much less common for many coronary situations |
How Drug-Eluting Stents Work (The “Tiny Pharmacy” Breakdown)
When a stent is placed, it solves the immediate problemimproving blood flow by propping open the artery. But
the artery still has to heal from the procedure. Healing is usually good. Healing that goes a little overboard?
That’s when trouble starts.
The Core Problem: Why Restenosis Happens
Angioplasty and stent placement mildly injure the inside of the artery. The body responds with a healing process
that can include inflammation and growth of smooth muscle cells. If too much tissue grows inside the stent,
it can crowd the artery’s openinglike weeds taking over a garden bed. That tissue overgrowth is one of the main
drivers of in-stent restenosis.
The DES Solution: Controlled Drug Release to Calm Tissue Overgrowth
A drug-eluting stent is built with three main “jobs” working together:
- Scaffold: The metal frame expands and holds the artery open.
- Coating system: A polymer (or other surface technology) helps hold the drug and control how it releases.
- Medication: An antiproliferative drug slows down the kind of cell growth that can lead to restenosis.
In practical terms, the stent releases a small amount of medication directly where it’s neededat the artery wall.
That local delivery is the big advantage: it targets the healing zone without trying to medicate your entire body
for a very specific patch of artery.
What Drugs Are Used in Drug-Eluting Stents?
Different stents use different medications, but many modern coronary DES use drugs in families that limit smooth
muscle cell proliferation. Commonly discussed examples include “-limus” drugs such as
sirolimus, everolimus, and zotarolimus. (Older designs also included other antiproliferative drugs.)
What About the Polymer Coating?
The coating is not just “paint.” It’s a delivery system. Think of it like a time-release capsule for the artery wall.
Different DES designs may use:
- Durable polymers that stay on the stent
- Bioabsorbable polymers that break down over time
- Polymer-free approaches that still control drug release through other engineering tricks
The design goal is to deliver the drug at a controlled ratefast enough to reduce problematic tissue growth,
but compatible with safe healing and long-term stent performance.
How a Drug-Eluting Stent Is Placed (Step-by-Step, Human Version)
Most drug-eluting stents are placed during PCI in a cardiac catheterization lab. The procedure is minimally invasive,
but it’s still a Big Deal (capital letters intentional) because it involves the coronary arteries.
Before the Procedure
- You may have blood tests, an ECG, and imaging or stress testing leading up to PCI.
- Your care team reviews medicationsespecially blood thinners, diabetes meds, and allergy history.
- Access site planning: many PCI procedures use the wrist (radial artery) or groin (femoral artery).
During the Procedure
- Access and catheter placement: A catheter is guided through an artery toward the heart.
- Coronary angiography: Contrast dye helps the cardiologist see where blood flow is narrowed.
- Balloon angioplasty: A balloon inflates to open the narrowed area.
- Stent deployment: The drug-eluting stent expands (often with the balloon), then stays in place as a permanent scaffold.
- Confirmation: Imaging confirms blood flow is improved and the stent is positioned correctly.
After the Procedure
Some patients go home the same day; others stay overnight depending on the reason for PCI (for example, heart attack
versus stable symptoms), the complexity of the procedure, and individual risk factors.
Why DES Usually Reduce Repeat Narrowing (And Why That Matters)
The “success” of a stent isn’t just the moment it opens the artery. It’s what happens in the weeks and months after.
Drug-eluting stents were developed because earlier approaches had higher rates of restenosis, leading to repeat procedures.
What “Better” Often Looks Like
- Fewer repeat procedures to reopen the same spot
- Less recurrent angina caused by re-narrowing in the stented segment
- More durable improvement in blood flow for many patients
That said, restenosis can still happen. It’s simply less common with many modern DES compared with older approaches,
and management options have expanded (including specialized techniques and, in select cases, drug-coated balloons).
Risks and Tradeoffs: The Two Big WordsClotting and Bleeding
Every medical device is a trade. A drug-eluting stent can reduce restenosis, but it also changes how the body heals
around the stentmeaning clinicians pay close attention to clotting risk, especially early on.
Stent Thrombosis: The “Don’t Ignore This” Risk
Stent thrombosis is a blood clot forming in the stent. It’s uncommon, but serious.
That’s one reason antiplatelet medications are a major part of the plan after DES placement.
Dual Antiplatelet Therapy (DAPT): Why It’s So Important
After PCI with a drug-eluting stent, many people are prescribed dual antiplatelet therapy:
typically aspirin plus a P2Y12 inhibitor (such as clopidogrel, prasugrel, or ticagrelor). This combination helps reduce
the risk of clotting in or near the stent while healing is underway.
How long DAPT lasts depends on factors like why the stent was placed (stable coronary disease vs. acute coronary syndrome),
bleeding risk, the specific stent and anatomy, and your overall clinical situation. Translation: it’s not one-size-fits-all,
and you should never stop these medications without your cardiology team’s clear instructions.
Bleeding Risk: The Other Side of the DAPT Coin
Antiplatelet therapy lowers clot risk but can increase bleeding risk. That may affect decisions about:
- Upcoming surgeries or dental procedures
- History of gastrointestinal bleeding or high bleeding tendency
- Other medications (including certain anti-inflammatory drugs)
- Whether shorter or longer DAPT duration makes sense
Who Might Get a Drug-Eluting Stent?
A drug-eluting stent may be recommended for coronary artery disease causing symptoms (like angina) or for emergency
treatment during certain heart attacks. Interventional cardiologists choose a strategy based on:
- Artery anatomy (vessel size, location, lesion length)
- Clinical context (stable symptoms vs. acute coronary syndrome)
- Ability to take antiplatelet therapy (including adherence and bleeding risk)
- Other health factors (kidney disease, diabetes, need for future procedures)
When the Conversation Gets More Nuanced
There are situations where the care team may discuss alternatives or additional planninglike if someone has a very high
bleeding risk, needs a major surgery soon, or has complex coronary disease where bypass surgery (CABG) might offer a better
long-term strategy. The “best” choice depends on the person, not just the artery.
Recovery and Long-Term Care: What Helps a Stent “Age Gracefully”
Think of the stent as a repairand your lifestyle and medication plan as the maintenance schedule that keeps that repair
from getting wrecked by the same forces that caused the problem in the first place.
Common Recovery Timeline (General)
- First days: access-site soreness (wrist or groin), fatigue, medication adjustments
- First weeks: gradual return to activity, possible cardiac rehab referral, follow-up visits
- Months onward: focus on risk-factor control (cholesterol, blood pressure, diabetes, smoking)
Cardiac Rehab: The Underrated MVP
Cardiac rehabilitation combines supervised exercise, education, and coaching. It’s not just “gym class with heart monitors.”
It can help rebuild stamina, improve confidence, and support long-term lifestyle changes that protect the coronary arteries.
Medication Adherence: The “Unsexy” Superpower
The single most important practical tip many clinicians repeat is also the least exciting:
take your antiplatelet medications exactly as prescribed. If side effects, cost, or confusion pop up,
call your cliniciandon’t improvise.
Frequently Asked Questions
How long does a drug-eluting stent release medication?
Drug release varies by stent design. Many DES are engineered to release medication over a controlled period after implantation,
targeting the higher-risk window for restenosis-related tissue growth. Your cardiologist can tell you the general expectations
for the specific stent used.
Can I feel the stent inside my heart?
Nopeople don’t feel the stent itself. What people may notice is recovery from the access site or improvement in symptoms
(like less chest pressure with activity), depending on the situation.
Are drug-eluting stents “safe”?
Drug-eluting stents are widely used and have a long track record in modern cardiology. Like any medical therapy, they have
risks and benefits, and safety depends on appropriate patient selection and good follow-throughespecially with antiplatelet therapy.
What symptoms should make me seek emergency care after stenting?
Seek urgent medical attention for chest pain/pressure that doesn’t go away, severe shortness of breath, fainting, or other
symptoms that feel like a heart emergency. If you’re unsure, it’s better to get checked than to “wait it out.”
Key Takeaways
- Drug-eluting stents keep arteries open and release medication to reduce restenosis risk.
- The drug and coating system are designed to control tissue overgrowth during healing.
- Dual antiplatelet therapy (DAPT) is a major part of staying safe after DES placement.
- Recovery is often smooth, but long-term success depends on risk-factor control and follow-up care.
Experiences: What It’s Like in Real Life (Patients, Families, and Clinicians)
“What does it feel like?” is usually the first question people asksometimes out loud, sometimes in the quiet panic
that shows up at 2:00 a.m. on a search engine. While everyone’s situation is different, there are some common experiences
that pop up again and again when people go through PCI with a drug-eluting stent.
Before the procedure, the emotional roller coaster is real. Many patients describe a strange mix of
relief (“Finally, we’re fixing the problem”) and fear (“They’re… going to my heart”). Families often ride a parallel track:
trying to stay calm, trying to be helpful, and secretly Googling everything they promised they wouldn’t Google.
A helpful mental reframe is that PCI is highly standardized. The cath lab team does this all the timelike a pit crew,
but with more monitors and fewer energy drinks.
During the procedure, many people remember sensations more than pain. Patients commonly report feeling
pressure at the access site and occasionally a brief chest pressure when the balloon inflatessomething clinicians often
warn about ahead of time so it’s less alarming. If the wrist is used, people may notice stiffness or soreness afterward,
plus the odd experience of realizing their “heart procedure” left them with what feels like a cranky wrist sprain.
(The heart is dramatic like that.)
After the procedure, the medication routine becomes the main character. It’s common to go home with a
new lineup: aspirin, a P2Y12 inhibitor, a statin, and possibly blood pressure or anti-anginal medications. Patients often say
the hardest part isn’t taking pillsit’s the mental load of making a mistake. Many set phone reminders, use weekly pill boxes,
or ask a family member to do a quick “med check” at dinner. Clinicians love these strategies because missing dosesespecially
early oncan raise clot risk. In real life, the best plan is the plan you’ll actually follow.
Symptom-wise, improvement can be immediateor subtle. Some people notice right away that stairs feel easier.
Others don’t feel dramatically different because their symptoms were intermittent, or because the stent was placed during a heart
attack and recovery includes the heart muscle healing too. This is where cardiac rehab can be a confidence booster: it helps people
trust their bodies again in a structured, supervised setting.
Clinicians experience DES decisions as a balancing act, not a single choice. From the care team’s perspective,
the stent is only part of the strategy. The bigger questions are: Can the patient safely stay on antiplatelet therapy? Is bleeding
risk high? Is there a planned surgery? What’s the anatomy like? Interventional cardiologists often talk about the “whole patient”
because the “best stent” on paper isn’t best if the aftercare plan doesn’t fit the patient’s reality. Good outcomes come from good
matchingmedical needs + life constraints + a plan that makes sense in a normal week, not just in a textbook.
Finally, many patients describe a lasting mindset shift: the stent feels like a second chance, but not a magic shield.
The most successful long-term stories usually include the unglamorous winstaking meds consistently, showing up to follow-ups,
addressing cholesterol and blood pressure, stopping smoking if applicable, and building a sustainable activity routine.
It’s less “movie montage” and more “steady playlist,” but it works.